
How Does an AI Doctor Work? A Plain-English Look Under the Hood
An AI doctor does not «know» what is wrong with you the way a physician does. It reads your words, matches them against patterns learned from medical text, and returns a ranked list of possible causes plus a sense of how urgent they are.
This guide explains, in plain English, what happens between the moment you type «sharp chest pain for two hours» and the moment the tool answers — and, just as important, where the technology stops.
Medical disclaimer: This article is for general information only. It is not medical advice and not a substitute for a licensed physician. If you think you are having a medical emergency, call 911. In a mental-health crisis, call or text 988 (US Suicide & Crisis Lifeline).
What an AI Doctor Actually Does, Step by Step
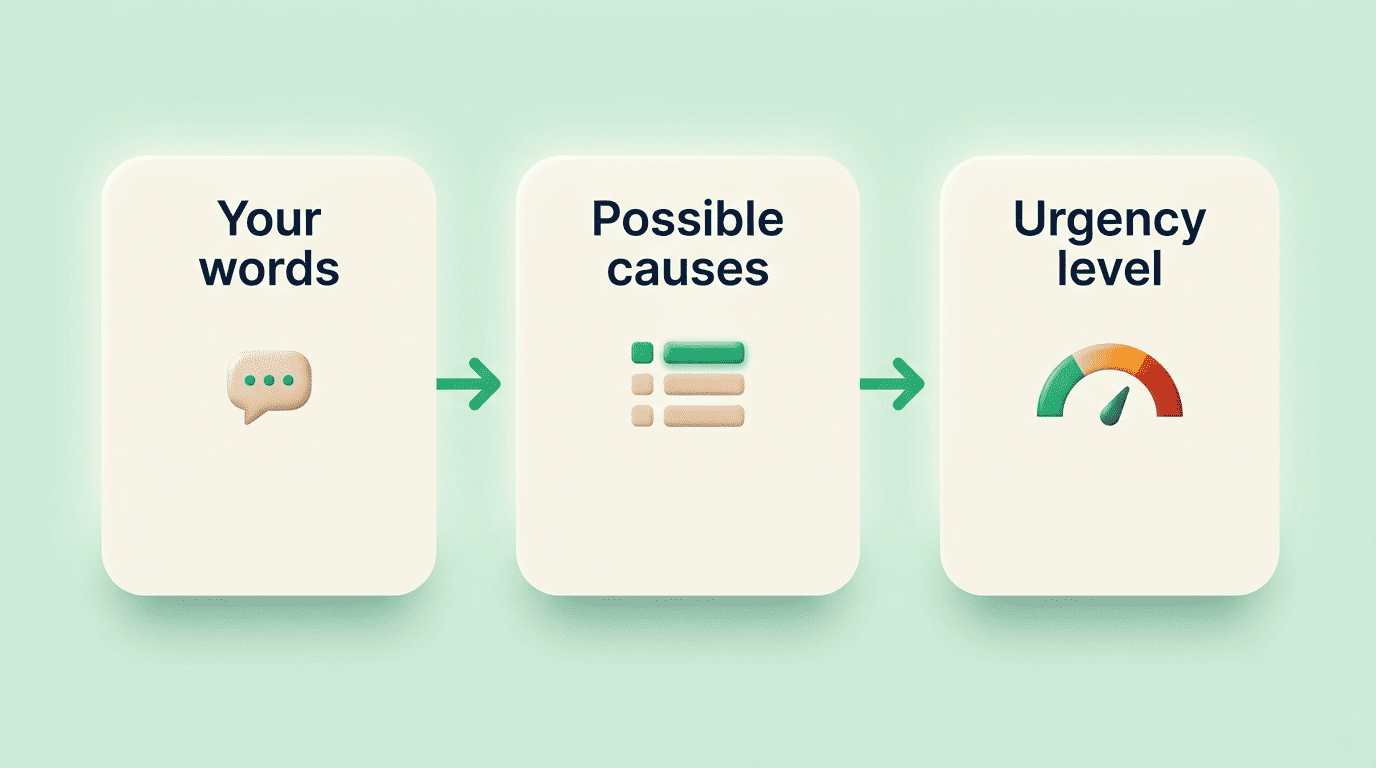
An AI symptom checker works in three connected stages, and understanding them makes it much easier to judge what the output is actually worth. None of the three stages involves the system examining you, testing you, or verifying anything against your actual body — it is working entirely from the words you supply.
From your words to structured symptoms
The tool uses natural language processing — usually a large language model — to turn free text like «I’ve had a throbbing headache and blurred vision since this morning» into structured clinical concepts: onset, location, severity, duration. It then asks follow-up questions, much like an intake nurse, to fill in the gaps you left out.
It helps to be blunt about what this step is and is not. It is pattern-matching on language: the model has seen millions of similar sentences paired with likely meanings, and it is predicting what your sentence probably describes. It is not understanding your body the way a nurse taking your pulse would.
Ranked possible causes (a «differential»)
Once your symptoms are structured, the AI medical assistant compares that pattern against thousands of documented symptom-to-condition relationships and returns a differential diagnosis — a ranked list of possible causes, most-likely first, not a single verdict.
That distinction matters more than it sounds. A differential is a list of things worth discussing with a clinician, not an answer. Two people with nearly identical symptom descriptions can end up with a different top item on their list, because the model weighs several factors at once:
- Age and sex
- How long symptoms have lasted and how they started
- Related symptoms mentioned in the same conversation
- Known conditions or medications you disclosed
That is exactly why the output is framed as possibilities to discuss, rather than a conclusion.
Assigning urgency (triage)
Separately from «what might this be,» the digital triage system estimates how soon you should act: self-care, see a doctor soon, or seek emergency care now. Safety rules flag red-flag combinations and push you toward emergency guidance rather than a differential list. Typical red flags include:
- Chest pain combined with shortness of breath
- Sudden weakness, numbness, or confusion (possible stroke)
- Severe difficulty breathing
- Signs of sepsis, such as high fever with a fast heart rate and confusion
- Thoughts of self-harm or suicide
If any of these apply to you right now, stop reading and call 911, or call or text 988 for a mental-health crisis.
What an AI Doctor Is Trained On
An AI doctor learns from large bodies of peer-reviewed medical literature, published clinical guidelines, and de-identified patient records, pairing described symptoms with documented outcomes so the underlying machine learning and neural networks can recognize patterns. The training data typically pulls from several categories at once:
- Peer-reviewed medical journals and research papers
- Professional society clinical guidelines
- De-identified electronic health records
- Structured symptom-to-condition databases used in clinical decision support
The World Health Organization has cautioned that training data for health AI can carry bias baked in from the populations and settings it was collected in, so data quality and human oversight matter as much as the size of the dataset. That caution is one reason vendors retrain and re-validate these systems against human clinicians rather than treating a single training run as finished.
It is worth being plain about what «learning» means here. The AI doctor is not reasoning from first principles about your anatomy or physiology; it is estimating what usually follows a given pattern of words in its training data. That approach is powerful for common presentations — a runny nose, a sprained ankle — and fragile for anything rare, atypical, or spread across multiple body systems at once.
How Accurate Are AI Symptom Checkers? What the Evidence Says
Independent evidence tells a more mixed story than marketing copy usually suggests, and the numbers are worth sitting with before you lean on any single result.
The numbers, honestly
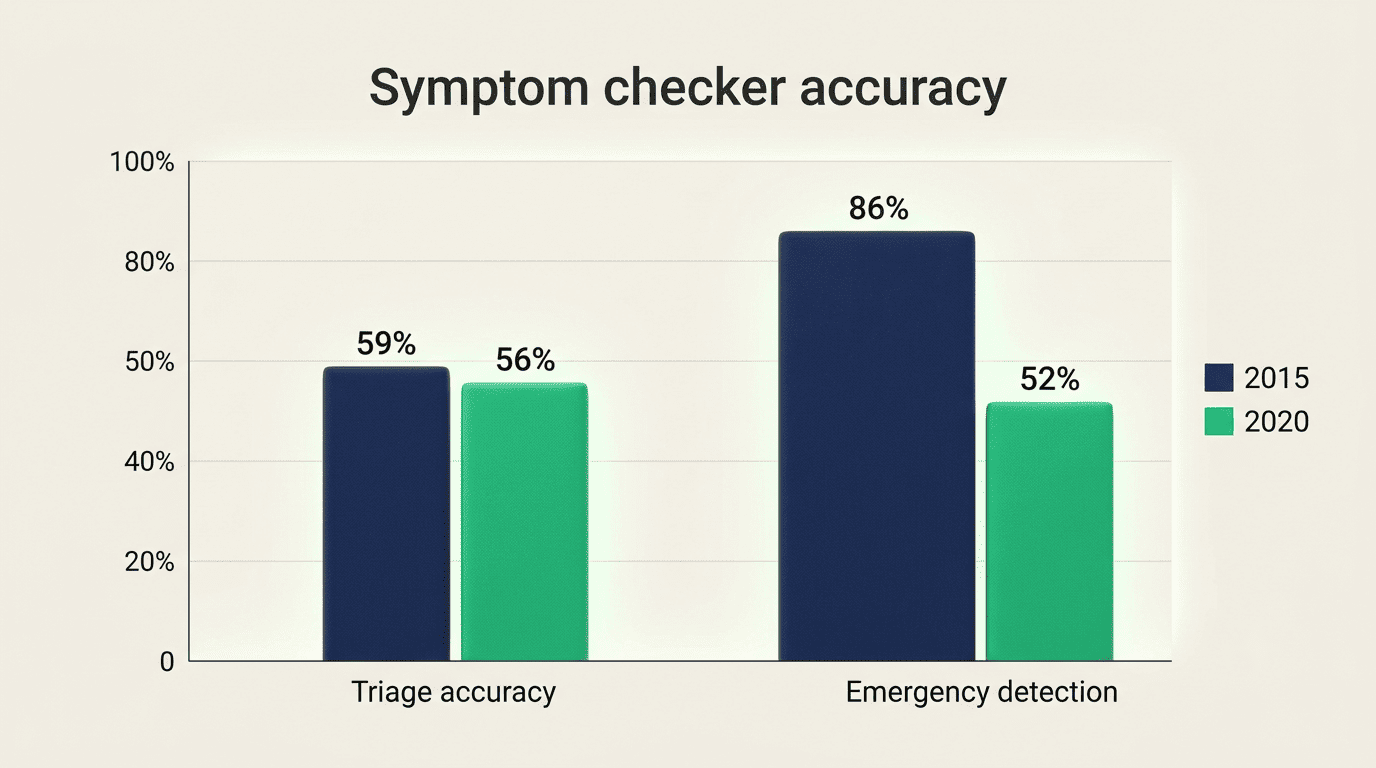
A peer-reviewed evaluation published in the Journal of Medical Internet Research and indexed by the NIH’s PMC tested 22 symptom checkers against 45 standardized case vignettes. Median triage accuracy was 55.8% in 2020 versus 59.1% in 2015 — no meaningful improvement over five years — and emergency-detection sensitivity actually fell from 85.7% to 51.9% over the same period.
«Triage performance of symptom checkers has, on average, not improved over the course of 5 years.»
Triage Accuracy of Symptom Checker Apps, JMIR (NIH/PMC)
That drop in emergency sensitivity is the single most important number in this section, because it is precisely the failure mode that safety rules and red-flag detection are meant to catch.
Good at common, weak at rare
Only 4 of the 22 apps tested — Mayo Clinic’s tool, Ada, Isabel, and Healthwise, or about 18% of the field — beat non-expert laypeople at telling emergencies apart from non-emergencies. Vendors commonly report roughly 70–80% accuracy for straightforward, common problems, but that figure is vendor-reported and unverified by an outside study, so it should be read as a marketing claim rather than independent evidence. Getting the likely condition right does not mean getting urgency right either: among cases where the app correctly identified the underlying condition, about 37.6% still received the wrong triage level.
| Study finding | Number |
|---|---|
| Symptom checkers tested | 22 |
| Case vignettes used | 45 |
| Median triage accuracy, 2020 | 55.8% |
| Median triage accuracy, 2015 | 59.1% |
| Emergency-detection sensitivity, 2020 | 51.9% |
| Emergency-detection sensitivity, 2015 | 85.7% |
| Apps beating laypeople on emergency vs. non-emergency | 4 of 22 (18%) |
| Correctly diagnosed cases with wrong triage | ~37.6% |
The Limits: Hallucination, No Physical Exam, and Bias
Hallucination and confident wrong answers. Because a large language model predicts plausible text rather than verified fact, it can produce a confident but incorrect answer — commonly called a hallucination. The system has no built-in way to know it is wrong, which is exactly why outputs need human review before anyone acts on them.
No exam, no tests, no context it wasn’t told. An AI doctor cannot listen to your lungs, feel your abdomen, order blood work, or notice what you didn’t think to mention. It is blind to everything outside the words you actually give it, which is a core reason it cannot diagnose you the way a physical exam and lab panel can.
Prompt sensitivity and inconsistent answers. The same underlying symptoms, described in slightly different words, can produce a different ranked list or a different urgency level. That sensitivity to phrasing is a known weakness of language-model-based tools, not a bug specific to any one app.
Bias inherited from training data. If the records, journals, or guidelines a model trained on underrepresent certain populations or symptom presentations, the model’s pattern recognition inherits that gap — a concern regulators and researchers continue to flag as these tools scale.
Put together, here is what an AI doctor cannot do, no matter how good its answers sound:
- Listen to your heart or lungs, or feel your abdomen
- Order or interpret blood work, imaging, or other tests
- Reliably catch a rare or atypical presentation
- Guarantee its ranked list or urgency level is correct
- Replace the judgment of a licensed physician
Why an AI Doctor Doesn’t Replace Your Doctor
An AI doctor is honestly positioned as a tool for triage and questions, not a verdict. The two sections below cover what that role looks like in practice and how oversight is supposed to keep it that way.
A tool for triage and questions, not a verdict
The realistic role is narrower than «diagnosis»: an AI doctor helps you understand a symptom, gauge urgency, decode a lab term, or prepare questions for a real appointment. It informs the conversation with a licensed clinician; it does not close it. Used this way, it can genuinely save time before a visit — describing what you noticed, when it started, and what makes it better or worse — without pretending to replace the exam that follows.
Here is a simple way to use one responsibly:
- Describe your symptoms in plain, specific language — onset, location, severity, what makes it better or worse.
- Read the ranked list of possible causes as options to discuss, not a diagnosis.
- Pay close attention to the urgency level the tool assigns, and treat any emergency flag as final.
- Write down the questions it suggests for your actual appointment.
- Book the visit, call a nurse line, or go to urgent care if the tool — or your own judgment — says something is off.
- If symptoms are severe, sudden, or worsening at any point, skip the app and call 911, or call or text 988 for a mental-health crisis.
Oversight and regulation
The strongest systems keep a human physician in the loop, and where a platform functions as a medical device, it must meet FDA requirements for AI-enabled medical devices. Mayo Clinic, one of the few organizations whose own symptom checker outperformed laypeople in the NIH-indexed study above, similarly frames these tools as a starting point for a conversation with a clinician rather than a replacement for one.
| AI doctor / symptom checker | In-person doctor visit | |
|---|---|---|
| Physical exam | No | Yes |
| Lab tests, imaging | Cannot order directly | Can order and interpret |
| Speed | Immediate | Hours to days for an appointment |
| Output | Ranked possible causes + urgency level | Diagnosis and treatment plan |
| Best for | Understanding a symptom, prepping questions | Confirming a diagnosis, treatment |
| Emergency handling | Flags red flags, directs to 911 | Provides direct emergency care |
Repeat the safety line, because it matters more than any accuracy number: for anything severe, sudden, or worsening — or any emergency — contact a licensed professional or call 911. For a mental-health crisis, call or text 988.